By: Graciella Davi & the NYCRA-NEWS Editorial team
Historically, there is substantial evidence of gross disregard and dismissive response on the part of the medical establishment in the way women have been diagnosed. Critics have speculated a vast array of reasons for this ‐ from professional carelessness and laziness to blatant sexism (and other forms of discrimination) to a lack of updated education in current research. But whatever the reasons may be, the lack of performance and attention in the hands of the medical diagnostician have resulted in tremendous danger to the patient. The most extreme cases of this underdiagnosing led to major health disorders and even death due to false negatives and missed conclusions from physicians and radiologists.
GILDA’S PLIGHT: “YOU’RE FINE…IT’S ALL IN YOUR HEAD”Our report starts with the legendary story of the late comedienne, Gilda Radner who died of ovarian cancer remission. In 1985, at a time when little information was available about this cancer, Ms. Radner started reporting pain in the upper legs and severe fatigue to her physicians'‐ whose diagnoses did not offer any satisfactory answers. Her recurrent issues worsened and she pursued other doctors for answers, some were said to have deemed her issues as 'mentally manifested'. By late 1986, her case had become so evident ‐ in the form of a grapefruit‐sized tumor from her abdomen, that she immediately underwent surgery and had a hysterectomy.
The medical community unanimously states the success of any cancer treatment is about TIME. "The earlier you catch it, the better your chances are of beating it". The size of her tumor was a sign of significant medical neglect to her issue, that by the time of her hysterectomy, her cancer was already at stage IV. [1]
Gilda Radner's story carries many survivorship lessons, including the need to stay proactive about (your) cancer. Her journey also shows the importance of getting a second opinion, research for all diagnostic care options and staying vigilant about your continued health through early detection. But her story remains a landmark to all awareness crusaders who identify and expose this unfortunate trend that continues to plague women in health crisis to this day.
From a 2018 documentary called
“Love, Gilda” (by Lisa D'Apolito), executive producer Meryl Goldsmith delivered a powerful and exclusive portrayal of the groundbreaking comic’s impact in our society as an entertainer and as one of the most powerful figures in cancer patient advocacy and survivorship. Ms. Goldsmith’s dedicated research on the life of Gilda Radner deeply explored her personal struggles including those pertaining to her health‐ leading to her untimely demise. "It's devastating to Gilda's family, friends, and fans, that she was not truly listened to when she complained of pains to doctors. Although she did end up with doctors who did the best they could to treat her, unfortunately she was delayed from getting the dire treatment she needed. Treatment was not as advanced as it is today, but early diagnosis was and remains crucial. We will never know if she would be alive today if doctors would have listened and looked carefully so they could have diagnosed it sooner."
Gilda Radner's life story touched the world of entertainment but her desperate journey to seek medical help was cemented in the very core of patient advocacy to this day. "She couldn't get out of bed for days, and had pelvic cramping, so no doctor should have said "everything is fine" or that it was "psychological" because it obviously wasn't. We can only hope that lessons are learned so others are diagnosed and treated quickly, and don't suffer the same fate. Gilda's legacy as a loveable comedian and national treasure lives on, along with all of the Gilda's Clubs around North America that provide support for those with cancer and their families. We also hope the message for doctors, both male and female, to listen to medical complaints carefully, especially from women, whose issues seem to be disregarded more often, is passed on through generations as well."
The world lost Gilda Radner in May 20, 1989, but many life‐saving lessons continue to resonate throughout the medical and patient communities from her story. She is an inspiration to advocates who push for a personalized treatment strategy. Ms. Goldsmith’s research and her film’s depiction of Gilda Radner’s treatment course stands as a major reference for any patient who may undergo similar struggles in getting proper treatment or accurate diagnoses.
THE FALSE NEGATIVE
Over a decade after Gilda’s passing, Dr. Nancy Cappello (a startlingly similar case of professional inefficiency and neglect) was diagnosed with stage 3C breast cancer in 2004 from a mis‐read mammogram, concealed behind dense breast tissue. A false negative mammography scan unidentified a large 2.5 cm suspicious lesion, which was later found via ultrasound readings was confirmed to be stage 3c breast cancer. This same cancer had metastasized to 13 lymph nodes. This sparked Dr. Cappello to create the "Are You Dense?" Foundation‐ an international awareness crusade to better support dense breast diagnostics and initiatives pass legislation to enact laws requiring mammography centers to inform patients about their breast density and the associated cancer risks.

Dr. Cappello passed away on Nov 15, 2018, from secondary myelodysplastic syndrome (MDS), a bone marrow cancer that was a complication of her prior aggressive breast cancer treatments. But she ignited a legacy of fighting for improved policies, advancing imaging technologies and continued research to better address this health crisis that puts the est. 40% of the female population (women with dense breasts) at risk of a false negative readings or other dense‐breast related cancers.
An excerpt from Nancy’s Story: “ I call it the best‐kept secret ‐ but it WAS known in the medical community. I have dense breast tissue – and women like me (2/3 of pre‐menopausal and 1/4 of post-menopausal) have less than a 48% chance of having breast cancer detected by a mammogram. In November 2003 I had my yearly mammogram and my "Happy Gram" report that I received stated that my mammogram was "NORMAL" and that there were "no significant findings." Six weeks later at my annual exam in January, my doctor felt a ridge in my right breast and sent me for another mammogram and an ultrasound… "Why didn't the mammogram find my cancer?" It was the first time that I was informed that I have dense breast tissue and its impact on missed, delayed and advanced stage cancer. What is dense tissue, I asked? Dense tissue appears white on a mammogram and cancer appears white – thus there is no contrast to detect the cancer (It is like looking for a polar bear in a snowstorm). I asked my physicians (now I had a TEAM of them) why wasn't I informed that I have dense breast tissue and that mammograms are limited in detecting cancer in women with dense breast tissue? The response was "it is not the standard protocol."
The disorder or the cause may vary, but sad endings to stories like these remain common in our patient community. We stand at a major point in history when medicine offers the highest advancements in technological innovations and treatment options- if not for HUMAN ERROR, or the mis-management of those entrusted to give professional care. So perhaps the most important lesson from Gilda Radner and Nancy Cappello 's story is to stay vigilant and "follow your gut". If something continues to feel wrong, trust your feelings. Never forget; doctors work for YOU. Never be railroaded to doubting your own feelings. There are MANY answers to cancer and they are all just a mouse click away.
TECHNICAL REVIEW: READING SCANS RESPONSIBLY
By: Dr. Robert L. Bard
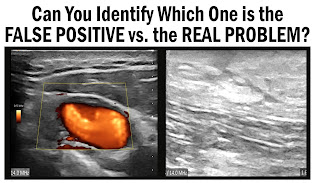
Nancy Cappello's "False Negative" led her late stage (type 3C) cancer, where the mammogram was not able to detect the cancer that was being concealed by her dense breast tissue. The lesson here is to upgrade the standard screening technology and expand to include supplemental scanning (such as the use of an ultrasound scan).
A "FALSE POSITIVE", on the other hand brings a different kind of crisis. It is the statistical classification in medicine referring to even less appealing terms like a MISREAD, an INACCURATE OVERSIGHT or a WRONG CONCLUSION. It is essentially a flaw in the patient diagnostic report that could cascade into the clinical team pursuing an inaccurately founded plan or the wrong path of care. My first commitment as a medical professional was in the US Air Force (1971) where I first witnessed the critical and sometimes even fatal results of 'false positive' reports and readings. Unnecessary surgical procedures were conducted and improper medications were dispensed- due to a possible misread of a scan or an inaccurate blood test. It was then that I realized the many potential types of disasters that could come from what could appear as a simple oversight- and what should be done to avoid them.
2021- the modern era of medical diagnostic advancements, and False Positives continue to happen much in the same way, due to the many 'flavors' of human error. But upon review of the "damage reports" from recent medical cases as a medical witness in a major malpractice case, it was concluded that NEGLIGENCE came from significant dependence and over-reliance on technologies to play a role in the clinicians' lack of discernment and focus.
Misdiagnoses offer their own set of problems as does the actual growth (cyst or tumor) that we are scanning for. Either HUMAN or TECHNICAL errors could lead to the wrong conclusion and distracts from the real pathology. Raising alarms of mis-reads have been known to put patients (and physicians) at great risk of unnecessary surgeries, costly testing and unwarranted treatments. What’s more, a false positive drives significant attention to the wrong area, where true issues and disorders are left unattended or found late when more damage occurs.
MASTERING THE ART OF INTERPRETATION
Suppose you misplaced your glasses and you can’t find them because the room is getting dark at sunset. You proceed to look for the glasses on all surfaces but if that doesn't work, you instinctively go deeper in your search (on shelves, coat pockets etc). Expert diagnostics involves thinking “outside the box” and the ability to "go deeper"- searching for what else is there or what item is missing.
Decades ago (as a junior radiologist) I was reviewing a spine xray and didn’t know what the abnormality was but I knew that somehow, it was not normal. So my gut told me to explore further. I took it to the neuro-radiologist at the Kansas City Medical Center near the McConnell Air Force Base who pointed out a bone curvature that was caused by a benign slow growing lumbar tumor that would eventually collapsed the spine and caused paralysis.

Unchaining the diagnostic thought process from standard textbook teachings opens up the possibility of deeper study. As a medical student in New York I was reviewing x-rays when my mentor, Dr Jack Rabinowitz, (head radiologist at Mt Sinai Medical Center) walked by and said, in passing, “nice example of pediatric metastatic neuroblastoma”. Amazingly, he immediately spotted the tumor purely from experience- what I did not recognize from my unseasoned eye. He explained how a baseball sized calcified mass on the kidney happens and slow growing cancers behave differently from aggressive, lethal tumors. As a large mass degenerates, it outgrows the blood supply and the dying tissue will calcify in the wall forming a shell of calcium on the x-ray. An untrained eye without this understanding would probably misinterpret these findings and offer a different report. The big take-away here is that professionals ranging in experience can sometimes get snagged by ASSUMPTIONS, but to continue exploring greater depths is what makes for a true cancer detective.
VIEWPOINTS:

CHRONIC FATIGUE & GETTING THE HELP WHEN YOU CALL OUT FOR IT
Cancer nutritionist and patient advocate Debbie Falborn, RN calls it "downright arrogant" of the many doctors who "brush off your feelings and your concerns... if you ask too many questions, you're a hypochondriac ‐ and if you complain too much about things they have no answers for, it's 'all in your head'. People die from this recipe of negligence!"
Among the many disorders that women have reportedly undergone struggles with getting help, Nurse Falborn also reviewed another (mostly) women related disorder; the confirmation of Chronic Fatigue Syndrome (CFS). "You have to persist… the patient's path to being taken seriously has been a long one‐ especially with symptoms that are tough to pinpoint and at a time when tests are limited." A 2019 Harvard Health article addressed the evolution in the medical community to be supported by over 9,000 scientific studies in 35 years to confirm this unusual health condition. It's official name is "Myalgic Encephalomyelitis" (ME/CFS) as has achieved data of over 2.5 million people affected in the United States. Its causes range from viral infections, immune system issues to physical/emotional trauma and causes a span of symptoms from extreme exhaustion to recurring headaches to enlarged lymph nodes in the neck & armpits.
It is apparent that science, technology and the medical community's desire to advance is truly upon us. Where current diagnostic resources are light years beyond where we were in the 80's and 90's, we are now able to find so many more answers to unique disorders once thought unfathomable. To instill better "detective work" on questionable unknowns (as part of medical due diligence) remains the clinical code of conduct of every physician and imaging specialist. Because of this, one can only hope to reduce or eliminate the level of negligence, false readings and (even) malpractice cases from underdiagnosed patients.
CONTRIBUTORS
SPECIAL THANKS
The publishers of NycraNews.com & Prevention101.org would like to give our heartfelt special thanks to Ms. Meryl Goldsmith, Executive Producer and Lisa D'Apolito Director of the documentary film "LOVE, GILDA", Joe Cappello (Co-founder of "Are You Dense?" Foundation), Dr. Robert L. Bard (www.BreastCancerNYC.com) and Debbie Falborn, RN (holistic cancer care advisor) for their valuable contributions, their insight and precious resources that have all led to the completion of this feature. Additional recognition goes to the technical advisement and unending "I'm just a phone call away" loving support of Julia Chiappetta and Jessica Connell-Glynn of the NY Cancer Resource Alliance and Dr. Noelle Cutter (Biology professor/Molloy College) for the countless collaborative hours of research, reference checking and shaping the voice of advocacy.
Our Friends & Supporters:
1) Gilda Radner/Illness: https://en.wikipedia.org/wiki/Gilda_Radner
2) Nancy's Story: https://www.areyoudense.org/stories/nancy/
4) Chronic fatigue syndrome: Gradually figuring out what’s wrong: https://www.health.harvard.edu/blog/chronicfatigue‐syndrome‐gradually‐figuring‐out‐whats‐wrong‐2019111418224
5) Video: Love Gilda- by Lisa D'Apolito (Magnolia Pictures/CNN Films): https://www.youtube.com/watch?v=1B44XRFotuo
Disclaimer & Copyright Notice: The materials provided on this website are copyrighted and the intellectual property of the publishers/producers (The NY Cancer Resource Alliance/IntermediaWorx inc., The AngioFoundation and Bard Diagnostic Research & Educational Programs). It is provided publicly strictly for informational purposes within non-commercial use and not for purposes of resale, distribution, public display or performance. Unless otherwise indicated on this web based page, sharing, re-posting, re-publishing of this work is strictly prohibited without due permission from the publishers. Also, certain content may be licensed from third-parties. The licenses for some of this Content may contain additional terms. When such Content licenses contain additional terms, we will make these terms available to you on those pages (which his incorporated herein by reference).The publishers/producers of this site and its contents such as videos, graphics, text, and other materials published are not intended to be a substitute for professional medical advice, diagnosis, or treatment. For any questions you may have regarding a medical condition, please always seek the advice of your physician or a qualified health provider. Do not postpone or disregard any professional medical advice over something you may have seen or read on this website. If you think you may have a medical emergency, call your doctor or 9-1-1 immediately. This website does not support, endorse or recommend any specific products, tests, physicians, procedures, treatment opinions or other information that may be mentioned on this site. Referencing any content or information seen or published in this website or shared by other visitors of this website is solely at your own risk. The publishers/producers of this Internet web site reserves the right, at its sole discretion, to modify, disable access to, or discontinue, temporarily or permanently, all or any part of this Internet web site or any information contained thereon without liability or notice to you.